Posterior Placental
Understanding posterior placental location is important for expecting parents and clinicians, since the position of the placenta can shape the pregnancy experience and influence monitoring decisions. In a posterior placental pregnancy, the placenta forms on the back wall of the uterus, which is a common and generally favorable placement that often supports normal fetal growth and movement.
What Is a Posterior Placenta
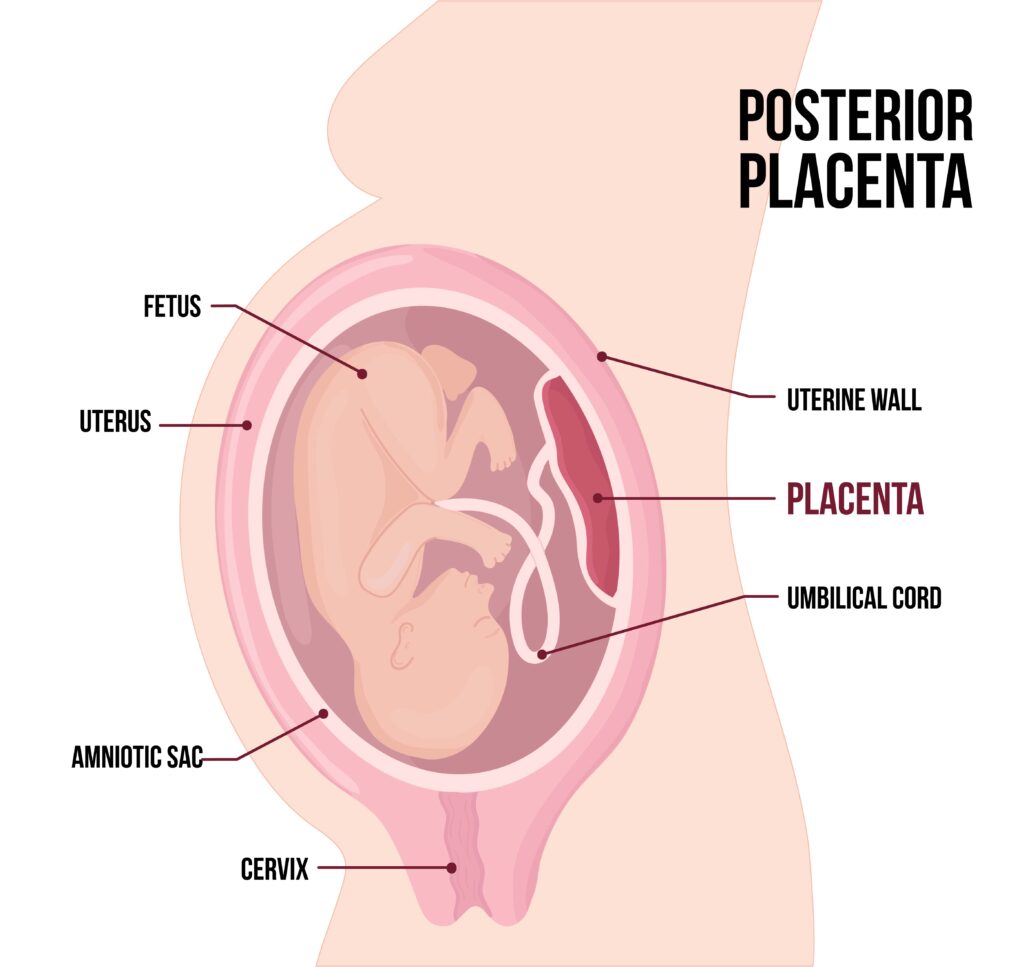
A posterior placental attachment means the placenta implants on the posterior wall, or back side, of the uterine cavity, opposite the baby's spine. This location is one of several placental positions, and it is typically classified as a grade 1 or 2 placenta on early scans before moving into a more mature posterior placental pattern as the pregnancy advances. Because the placenta sits toward the front of the mother's spine from the outside, it usually does not cover the cervix and is associated with a lower risk of placenta previa compared with other positions.
During routine anatomy ultrasounds, sonographers measure placental location and may note a posterior placenta when the placental edge is closest to the posterior uterine wall. This finding is recorded in medical notes and can affect choices about follow-up scans, especially if the placenta appears close to the cervix early in pregnancy. Most posterior placentas migrate and evolve normally, providing a supportive cushion for the baby without interfering with standard prenatal care.

Symptoms and Physical Sensations
Many people with a posterior placenta report feeling more pronounced kicks and movements in the front of the abdomen, because the placenta is positioned against the back wall and the baby is often facing forward toward the mother's belly. This can make fetal movements feel sharper and more distinct, particularly as the baby grows and has less cushioning between limbs and the abdominal wall. Some individuals also notice stronger sensations of pressure or stretching in the lower back, especially when the baby engages in a posterior or occiput posterior position during later pregnancy and labor.
While these sensations are common, they are not universal, and the absence of pronounced front-of-belly movements does not automatically rule out a posterior placenta. Healthcare providers rely on ultrasound confirmation rather than symptoms alone, since the exact placental location can only be reliably determined through imaging. Any new or concerning patterns of fetal movement, pain, or bleeding should be discussed promptly with a clinician, regardless of placental position.
Diagnosis and Imaging Techniques
Obstetric ultrasound is the primary tool for diagnosing a posterior placenta, using transabdominal and, when needed, transvaginal approaches to visualize the uterine wall and placental location. Early scans may simply note placental position as anterior, posterior, fundal, or lateral, while later detailed exams can refine this description and assess placental grade. A posterior placental location is often easier to evaluate in the second trimester, when the placenta has not yet fully expanded and fetal structures are clearly visible.
In some cases, providers may use additional imaging or follow-up scans if the placenta appears close to the cervix or if there are concerns about placenta accreta spectrum in individuals with risk factors such as prior uterine surgery. For most posterior placentas, however, routine prenatal ultrasounds and clinical exams are sufficient to track fetal growth, amniotic fluid levels, and placental maturity without invasive procedures.
Impact on Pregnancy and Delivery
A posterior placenta typically does not restrict fetal growth or limit the baby's ability to move, and many individuals with this placental position deliver healthy babies without complications. Because the placenta is on the back wall, it may sometimes delay the descent of the baby's head during labor, contributing to a longer first stage of labor or a higher likelihood of occiput posterior positioning at the time of delivery. Understanding this relationship helps clinicians plan for possible interventions, such as position changes or assisted delivery, when needed.
In most situations, a posterior placenta does not require cesarean birth unless other indications arise, such as fetal distress, failure to progress, or concurrent placenta previa. Care teams may recommend specific labor positions, such., as hands-and-knees or side-lying maneuvers, to encourage the baby to rotate into an anterior position. Continuous monitoring and open communication between the birthing person and providers support safe vaginal delivery even when the placenta is posterior.
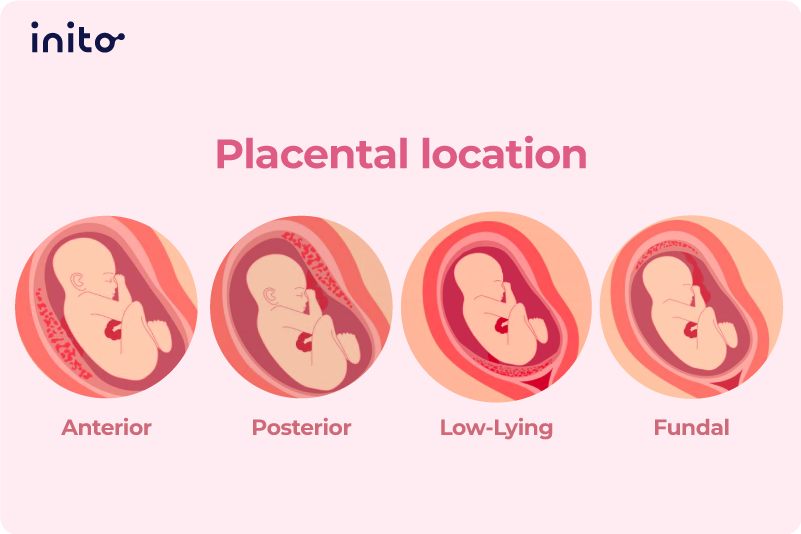
Comparison With Other Placental Positions
Anterior placenta placement means the placenta sits on the front wall of the uterus, which can cushion fetal movements and sometimes obscure hearing the heartbeat early on. By contrast, a posterior placental location often allows stronger perception of kicks and may facilitate earlier detection of fetal patterns on monitoring. Fundal placenta refers to a position at the top of the uterus, while lateral placenta indicates placement toward the sides, and each can have slightly different implications for symptom timing and delivery planning.
Placenta previa, where the placenta covers or is very close to the cervix, represents a more significant deviation from a typical posterior placental arrangement and usually necessitates modified delivery plans. Recognizing these distinctions helps patients understand their own placental reports and engage confidently in discussions about monitoring, timing of birth, and pain management options.
Tips for Comfort and Communication
Individuals with a posterior placenta may find that certain positions, such., as leaning forward on a birthing ball or using supportive cushions, alleviate back pain and encourage optimal fetal positioning. Gentle movement, prenatal yoga, and pelvic tilts can support the baby's rotation and reduce discomfort associated with a persistent occiput posterior presentation. Staying informed about placental location and asking questions during prenatal visits promotes shared decision-making and reduces anxiety.

Keeping a simple log of fetal movements, noting patterns of back pain, and discussing any concerns with a midwife or obstetrician can help ensure timely interventions if needed. A posterior placenta is common and usually straightforward, but personalized guidance from a trusted healthcare provider remains the best source of information throughout pregnancy and delivery.
Overall, a posterior placental location is a normal variant that typically supports a healthy pregnancy and vaginal birth. By understanding how this placental position influences sensations, imaging, and delivery planning, expecting parents can approach their care with clarity and confidence, focusing on safe outcomes and supportive partnership with their clinical team.
Posicionamento da placenta na ultrassonografia | Posicionamento placentário anterior/posterior/fu...
Posições da placenta no ultrassom | Posicionamento placentário anterior/posterior/fundal/lateral USG Casos incluídos ...
